

Updated science. Outdated care. Women paid.

In 2002, a single study changed how millions of women were treated for perimenopause. The science has since been corrected. The clinical behavior largely hasn’t.
If you’ve ever asked your doctor about hormone replacement therapy and been met with hesitation — or an outright no — there’s a good chance that response traces back to a study published more than two decades ago. Understanding what that study actually said, and what it didn’t, is one of the most useful things a woman in perimenopause can do for her health and her finances.
What the WHI study actually found
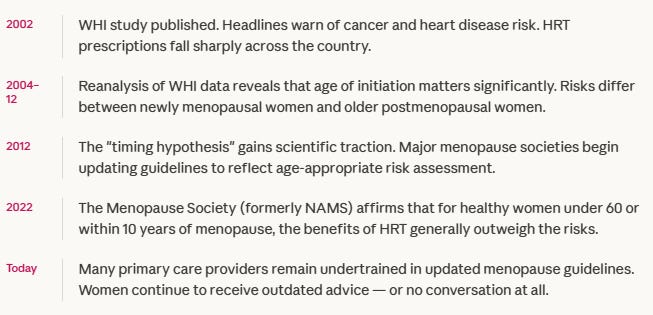
In 2002, the Women’s Health Initiative published findings that sent shockwaves through the medical community.
Headlines declared that HRT caused breast cancer and heart disease. Prescriptions dropped by half almost overnight. An entire generation of physicians became reluctant — or flatly unwilling — to prescribe hormones for menopausal symptoms.
Here’s what the headlines left out.
The WHI study used a specific formulation: oral conjugated equine estrogen combined with synthetic progestin (medroxyprogesterone acetate), given to women whose average age was 63 — well past the menopausal transition. Many participants had pre-existing cardiovascular risk factors. The study was not designed to evaluate HRT in perimenopausal women in their late 40s and early 50s. It was designed to test whether hormones could prevent chronic disease in older women who were already postmenopausal.
When researchers went back and analyzed outcomes by age, the picture shifted significantly. Women who began HRT close to menopause — within ten years of their final period, or before age 60 — showed a different risk profile entirely. In some analyses, early initiators showed reduced cardiovascular risk, not increased. The blanket warning that defined a generation of clinical practice did not hold up when applied to the population it was most often used to justify.
The science moved. The clinical culture didn’t keep up. Women paid the difference.
The cost of navigating outdated care
When a woman’s primary care physician isn’t current on menopause medicine, she has options — but none of them are free. Finding a provider who will have a real, evidence-based conversation about HRT often means stepping outside the standard care pathway.

The specialist shortage compounds this. Menopause-certified providers are concentrated in major metropolitan areas. Telehealth platforms have helped, but the most accessible ones often operate on subscription models that add another monthly line item. Women who can’t afford that path cycle through primary care appointments, get told their symptoms are “normal,” and go another year without answers.
That delay has downstream costs — in untreated symptoms that affect work performance, in bone density loss that begins in perimenopause and accelerates without hormonal support, in cardiovascular risk that estrogen was partly buffering against. The confusion tax isn’t just the money spent navigating a broken system. It’s the compounding cost of the years spent in it.
What you can do with this information
Knowing the history puts you in a stronger position in the exam room. A provider who cites the WHI as a blanket reason to avoid HRT is working from a 2002 headline, not 2026 evidence. You are entitled to ask which guidelines they’re using and when they last reviewed them.
The Menopause Society maintains a certified provider directory.

If your current provider isn’t able to engage with updated evidence, that’s information too. Finding someone who can may cost money upfront. Across a decade of undertreated symptoms, it is almost certainly the less expensive option.